35 YR OLD MALE WITH HYPOGLYCEMIA AND ALTERED SENSORIUM.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 35 year old male patient was brought to casuality with the chief complaints of :
Unresponsiveness since 4 am morning
Abdominal distension since 1 week
Pedal edema since 1 week
Yellowish discoloration of eyes.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 6 yrs back then he developed yellowish discoloration of eyes , swelling of both legs and abdominal distension, went to local hospital and diagnosed with Chronic liver disease.
Since then patient was on irregular medication and continued taking alcohol intermittently.(Patient is an known alcoholic since 20 years.)
History of increased bilateral pedal odema which is pitting in nature since 1 week .
History of increased abdominal distension since 1 week
Since 4 days, patient has c/o fever subsided after medication.
C/o loose stools 4-5 episodes per day,no h/o malena , pain abdomen
C/o nausea and loss of appetite
C/o altered sensorium not responding to commands
No h/o weakness and no h/o involuntary movements
PAST HISTORY:
He was diagnosed with Portal hypertension and Grade2 oesophageal varices.
Not a known case of HTN , DM , Asthma , Epilepsy.
PERSONAL HISTORY:
Diet - Mixed
Appetite - Decreased
Sleep - adequate
Bowel & bladder movements - Normal
Addictions - Regular intake of alcohol (180ml) since 20 years
FAMILY HISTORY:
No similar complaints in the family
GENERAL EXAMINATION:
Patient is conscious , coherent and cooperative &
Thin built and malnourished.
Icterus present

No pallor , cyanosis , clubbing and lymphadenopathy.
Bilateral pitting type of pedal odema present

Vitals:
Temp : Continuous at 100 F
BP : 100/80 mm Hg
PR : 105 bpm
RR : 25 cpm
GRBS : 33 mg/dl
SpO2 : 91% at Room air
SYSTEMIC EXAMINATION:
CVS : S1S2 + , No murmurs
RS. : BAE + , Normal vesicular breath sounds heard.
P/A : abdominal distension is presentAltered coagulation signs:



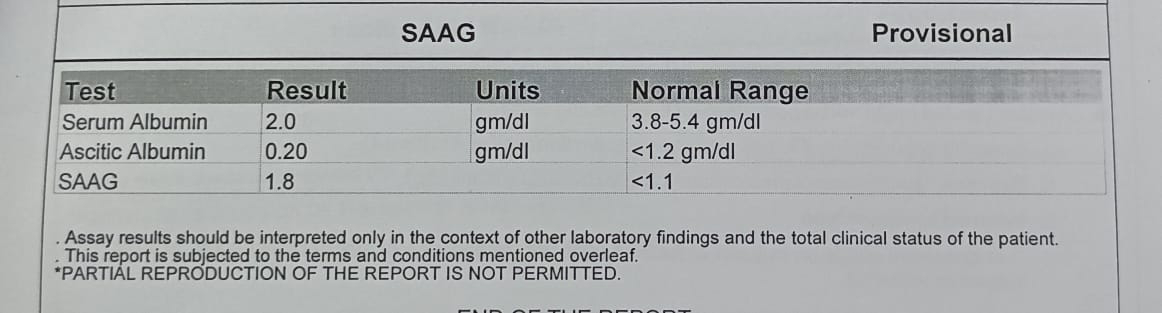
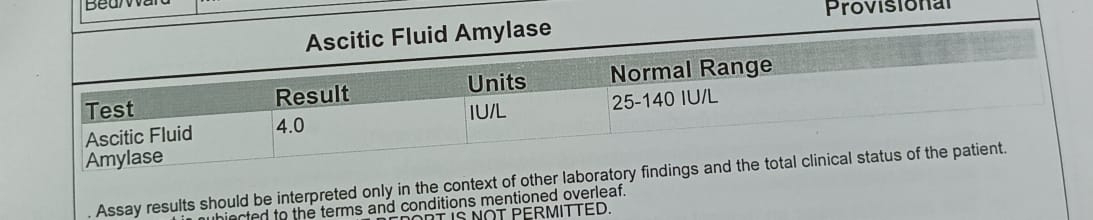
INVESTIGATIONS:











PROVISIONAL DIAGNOSIS:
HEPATIC ENCEPHALOPATHY SECONDARY TO LIVER FAILURE
RECURRENT HYPOGLYCEMIA
K/C/O CHRONIC LIVER DISEASE WITH GROSS ASCITES AND SPLENOMEGALY(PORTAL HTN)
Secondary bacterial peritonitis
Pre renal AKI (hepatorenal syndrome?)
Deranged coagulation time
TREATMENT:
INJ.LASIX 20 MG/IV/BD
TAB.ALDACTONE 50 MG/RT/BD
INJ.25% DEXTROSE 100ML/IV/SOS IF GRBS<60 MG/DL
SYP. LACTULOSE 20 ML/PO/BD
INJ. THIAMINE 1 AMP IN 100 ML NS/IV/TID
GRBS CHECK HOURLY
BP/PR/TEMP CHARTING HOURLY
T. UDILIV 300 MG/ RT/BD
SYP. HEPAMERZ 2 TBSP/RT/BD
T RIFAXIMIN 550 MG /RT/BD
ENEMA 12 TH HOURLY
STRICT I/O CHARTING
INJ.CEFOTAXIME 2G /IV/BD



Comments
Post a Comment